Occipital neuralgia and migraine are confused constantly, even by clinicians, because both can cause severe head pain with light sensitivity. But they are different conditions with different treatments, and telling them apart is the difference between months of relief and months of the wrong medication. This guide lays out the differences clearly, drawn from more than two decades of living with occipital neuralgia ourselves.

The Quick Answer
Occipital neuralgia is a nerve condition causing sharp, shooting pain from the base of the skull, with scalp tenderness and triggers related to neck movement and touch. Migraine is a neurological condition causing throbbing, often one-sided pain, usually with nausea and strong light and sound sensitivity. The simplest test: if pressing at the base of your skull reproduces the pain, it points to occipital neuralgia.
Side-by-Side Comparison
| Feature | Occipital Neuralgia | Migraine |
|---|---|---|
| Pain type | Sharp, stabbing, electric | Throbbing, pulsing |
| Where it starts | Base of skull, travels up | Temple, forehead or behind eye |
| Sides affected | One or both, follows nerve path | Usually one side |
| Scalp tenderness | Pronounced, base of skull | Possible but less specific |
| Nausea/vomiting | Rare | Very common |
| Main triggers | Neck movement, touch, posture | Light, hormones, food, stress |
| Duration | Seconds to hours, recurring | 4 to 72 hours |
Why the Distinction Matters
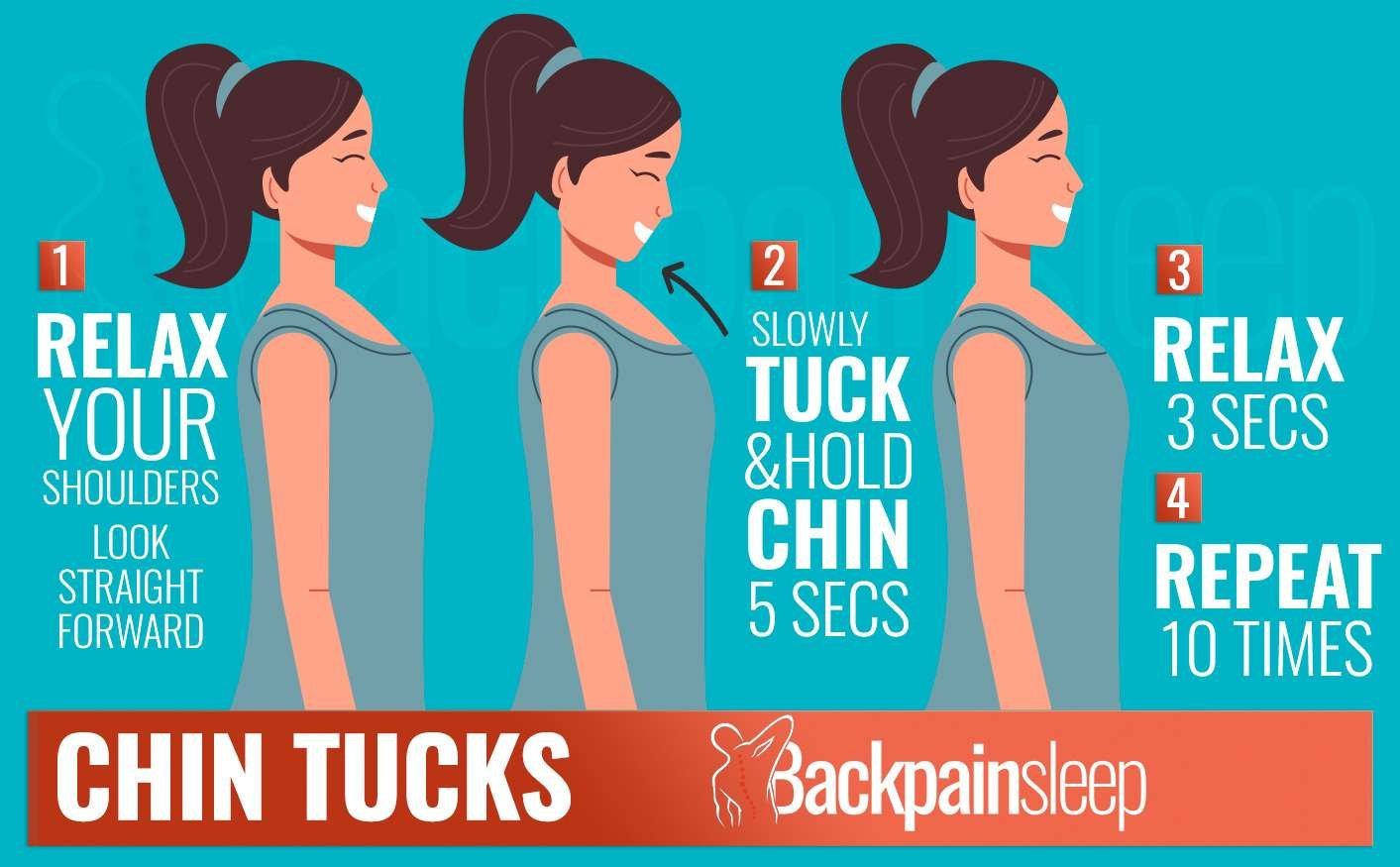
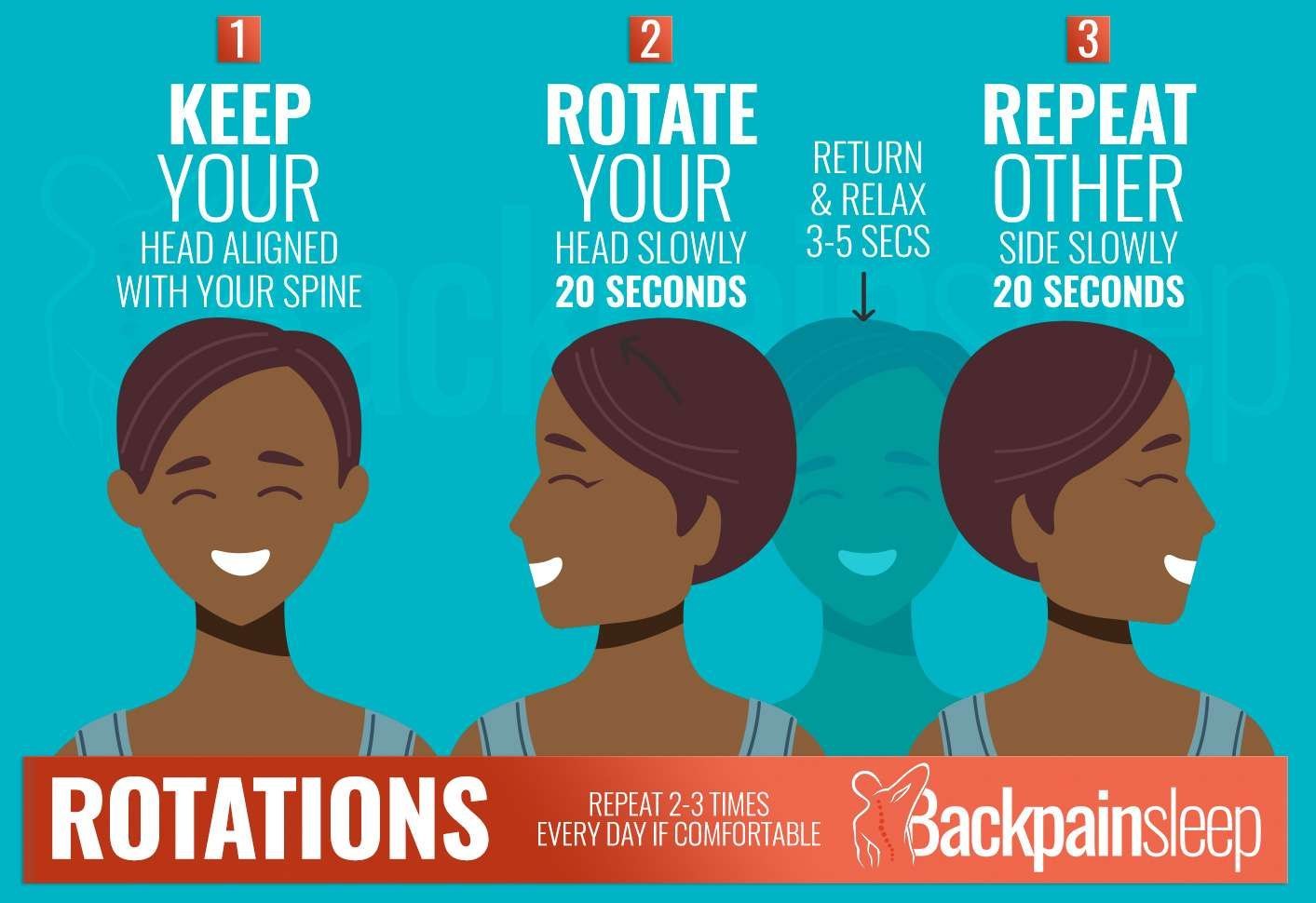
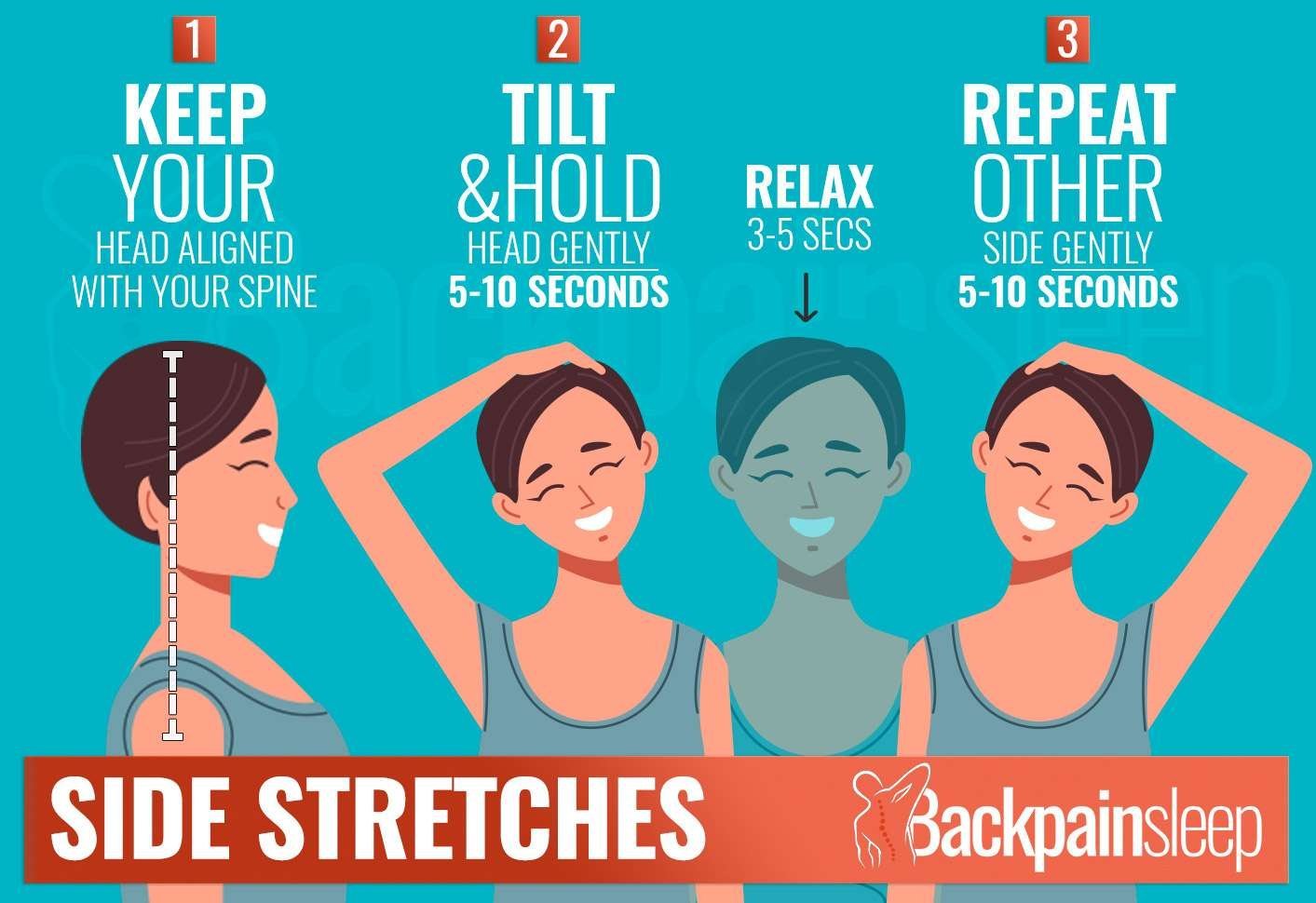
Migraine treatment focuses on triptans, preventive medication, and avoiding dietary and sensory triggers. Occipital neuralgia responds to physical approaches, posture, massage, a supportive pillow, and in stubborn cases nerve blocks. If you treat occipital neuralgia as a migraine, you may spend months on medication that does little, while the simple physical interventions that would actually help go untried. That is why getting the diagnosis right comes first.
The Scalp-Tenderness Clue
One of the most reliable distinguishing features is scalp tenderness at the base of the skull. With occipital neuralgia, the skin and scalp at the back of the head often become so sensitive that brushing your hair or resting on a pillow hurts, and pressing the spot where the nerve emerges reproduces the pain. Migraine does not usually produce this specific, localised tenderness. If you have it, occipital neuralgia is likely.
Can You Have Both?
Yes. The two can coexist, and occipital neuralgia can even trigger migraine-like symptoms in some people. This overlap is part of why diagnosis is tricky. If you suspect both, a neurologist can untangle them, often using a diagnostic occipital nerve block, which numbs the occipital nerve to see how much of your pain it accounts for. See our complete guide to occipital neuralgia for the full picture.
Frequently Asked Questions
Can occipital neuralgia be mistaken for a migraine?
Very often. Both cause severe head pain and light sensitivity. The distinguishing features are the sharp, shooting quality of occipital neuralgia pain and its origin at the base of the skull.
How do doctors confirm occipital neuralgia rather than migraine?
The most reliable test is an occipital nerve block. If a local anaesthetic injected near the occipital nerve relieves the pain, it confirms occipital neuralgia rather than migraine.
Does occipital neuralgia cause nausea like a migraine?
Rarely. Nausea and vomiting are typical of migraine, not occipital neuralgia. Their absence, combined with sharp pain from the base of the skull, points away from migraine.
Can the same treatment work for both?
Some overlap exists, stress and neck-tension management help both, but the core treatments differ. Migraine needs migraine-specific medication and trigger control; occipital neuralgia responds to physical and nerve-targeted approaches.
The information on this site is based on personal experience and research. It is not medical advice. Always consult a qualified healthcare professional for diagnosis and treatment.
Was this guide helpful?
Thank you. Your feedback helps us improve.